Article Text

Abstract
Doctors, patients, and their relatives face a complex decision when there are multiple treatment options that differ in their profiles of risk and benefit over time. Doctors from a single specialist paediatric cardiac unit participated in a correlational study that used a novel tool (subjective multi-state survival graphs) to elicit their beliefs about the likely outcome of different treatments. Doctors' preferences were more closely related to their beliefs about long term, rather than short term, outcomes. This is consistent with placing greater value on far future than on immediate life years, highlighting the importance of incorporating patients' values for these outcomes into decisions of this kind. Beliefs about likely outcomes differed with whether or not doctors encountered former paediatric patients who were now adults, illustrating the difficulty of deciding what risk information should be available when the evidence base on outcomes is limited. Some problems of risk communication are identified, and the value of multi-state survival graphs as an aid to communication is discussed.
- doctor preference
- risk
- informed choice
- decision making
- patient-caregiver communication
Statistics from Altmetric.com
Key messages
-
Doctors' treatment recommendations are consistent with selecting the option that maximises the chance of the best outcome, without necessarily minimising the chance of the worst outcome.
-
Doctors' beliefs about likely outcomes vary according to the patient groups they encounter, notably so for the long term outcomes that appear to be more important for determining preference.
-
Patients' outcome and time preferences may differ from those implicit in doctors' treatment recommendation and should be considered in decisions.
-
Risk communication is particularly problematic when the evidence base is limited or there are several options with many possible outcomes. In such situations, multi-state survival graphs may be an aid to communication.
Faced with several treatment options for their patient, why do different doctors recommend different options? If two doctors differ in their beliefs about the relative merits of different treatments, we would expect that they might differ in their treatment preferences. However, that begs a second question. What lies behind differences in belief about the relative merits of different treatments?
Management options for children with congenital heart disease vary in their profiles of risks and benefits over time. The probability of death following surgical intervention can be high. Such interventions may provide better long term prospects for survival or good heart function than strategies with a better chance of short term survival. This paper examines the relationship between doctors' treatment preferences and their beliefs about the likely outcomes of different management strategies. Specifically, what will receive greater weight when comparing two treatments with different risk/benefit profiles—differences in the perceived likelihood of immediate outcomes or of long term outcomes?
Of course, in this situation, it is not only the surgeon or physician who must wrestle with the choice between treatments. Parents need to be informed of the risks and benefits of treatment, and intervention is ultimately dependent upon their consent. A further development occurs when children are old enough to be informed of treatment risks and involved in the decision to operate. These issues resonate across a range of healthcare decisions. Adults with carotid artery stenosis also face a similar choice between surgery, with a better chance of long term survival, and medical management, with a better chance of short term survival.1 Providing clear information about treatment is an avowed aim within all areas of NHS provision,2 and a demanding characteristic of informed or shared decision making.34 The importance of involving patients' families extends beyond the paediatric setting to, for instance, end of life decisions.5 In this paper these generic issues of patient preference are considered together with some more specific questions relating to doctors' treatment preferences for children with congenital heart disease.
The clinical setting
“Univentricular hearts” are a family of congenital conditions in which the systemic and pulmonary circulations are supported predominantly by a single functioning ventricle. One palliation for this condition is the bidirectional Glenn (BDG) shunt where the superior vena cava is “disconnected” from the heart and “reconnected” directly to the pulmonary arteries, resulting in some improvement in systemic arterial saturation. A more aggressive palliation is the Fontan procedure which diverts the whole caval return to the lungs, offering patients full systemic saturation in return for a high systemic venous pressure. Current Fontan techniques generally consist of a BDG shunt plus a direct connection between the inferior vena cava and the pulmonary artery by constructing a “lateral tunnel” through the right atrium (total cavopulmonary connection, TCPC)6 or addition of an extracardiac conduit joining these two vessels.7 Recent practice has swung towards staging the operation, performing the BDG shunt first and undertaking the rest of the Fontan operation some years later. As long term complications following Fontan operations began to emerge, a debate developed as to whether the BDG shunt alone might be the preferred “definitive palliation” for univentricular hearts.89 The risk of early mortality associated with major heart operations means that there will be cases where all of the available surgical interventions are unattractive. Thus, for an individual patient, both no treatment and different surgical options are available and are considered in this study.
Variation in the manner in which patients are monitored in the years following surgery may play a part in differentially shaping individual doctors' beliefs about the relative merits of competing management strategies. Feedback has repeatedly been shown to play an important role in shaping judgement.10–12 However, the sparsity of published results for longer term outcomes following surgery in univentricular heart patients means that opinions about patient outcomes are formed under conditions of limited feedback, particularly if specialists see an exclusively paediatric clientele. Doctors who see adult patients (termed “Grown Up Congenital Heart (GUCH)” patients) would be expected to receive more feedback on long term outcomes. Anecdotally, some cardiologists working with GUCH patients argue that surgical interventions for univentricular hearts have worse long term outcomes than was anticipated by those who reported initial success with these interventions. If such views are common, “GUCH practitioners” (who see both children and GUCH patients) would be expected to be more pessimistic than their colleagues concerning the long term prospects following surgical intervention.
The study described here examines two main questions:
Are preferences between options more closely related to the perceived relative merits of these options in the long term or in the short term?
Can differences in the patient groups encountered by doctors account for differences in their belief about the relative merits of these options?
Method
DESIGN
Participants received a booklet with details of two patients for whom they estimated the chances of survival and of survival with “good heart function” for each of four possible courses of action. Each option was also rated. The first patient considered was young (approximately 3 years old) and the second one was older (17 years old). These ages are towards the extremes typically considered for the interventions under examination, allowing generalisation to patients of differing ages. There were two versions of the task booklet (A and B), each with different patients (matched by age). The purpose of this was to extend the generalisability of findings by avoiding reliance on one or two cases, without inflating the time for each participant to complete the task.
Patient summaries were drawn up using existing patient notes (box 1). Summaries were checked for accuracy by the consultant cardiologists responsible for their care, and piloted for clarity with an additional cardiologist or cardiac surgeon.
Box 1. Example of patient summary.
Patient 1: AL, 2 years 11 months, male
ANATOMY
Right atrial isomerism.
Common atrioventricular valve
Double inlet right ventricle, double outlet right ventricle
Anterior aorta, pulmonary atresia
Infradiaphragmatic totally anomalous pulmonary venous drainage
Right aortic arch
Small left superior vena cava with bridging vein to larger right superior vena cava
HISTORY
Premature (31 weeks)
Surgery at 15 days: repair totally anomalous pulmonary venous connection (direct anastomosis of pulmonary venous confluence to left atrium), 3.5 mm left modified Blalock-Taussig shunt, ligation of left and right arterial ducts
Re-exploration of shunt to confirm patency on the following day
Surgery at 1 year 1 month: 5 mm central shunt between ascending aorta and right pulmonary artery (left modified Blalock-Taussig shunt thrombosed)
CURRENT SYMPTOMS
Well but increasing cyanosis
INVESTIGATIONS (AT 2 YEARS 8 MONTHS)
(haemodynamic data supplied)
Patent shunt to central confluent pulmonary arteries
Pulmonary artery stenosis at site of shunt insertion
PARTICIPANTS
Thirteen doctors from the same tertiary referral centre participated. Seven identified themselves as cardiologists, three as surgeons, and one as from other specialties. Seven identified their grade as consultant and four as other. Eight indicated they saw GUCH patients in the course of their practice, whereas three indicated that they did not. The mean number of years in specialty was 9 years.
PROCEDURE
Data collection took place in a single session. Participants were psuedo-randomly assigned to receive one of two task booklets (A or B) by distributing booklets in an alternating order so that no two participants sitting next to each other received the same booklet. Before commencing the task, participants received a verbal orientation and were given a two page written introduction to the task.
For both patients, participants considered four possible courses of action:
Option 1: no further surgical intervention
Option 2: one stage TCPC
Option 3: a BDG shunt
Option 4: a BDG shunt now with TCPC completion in 5 years (two stage TCPC)
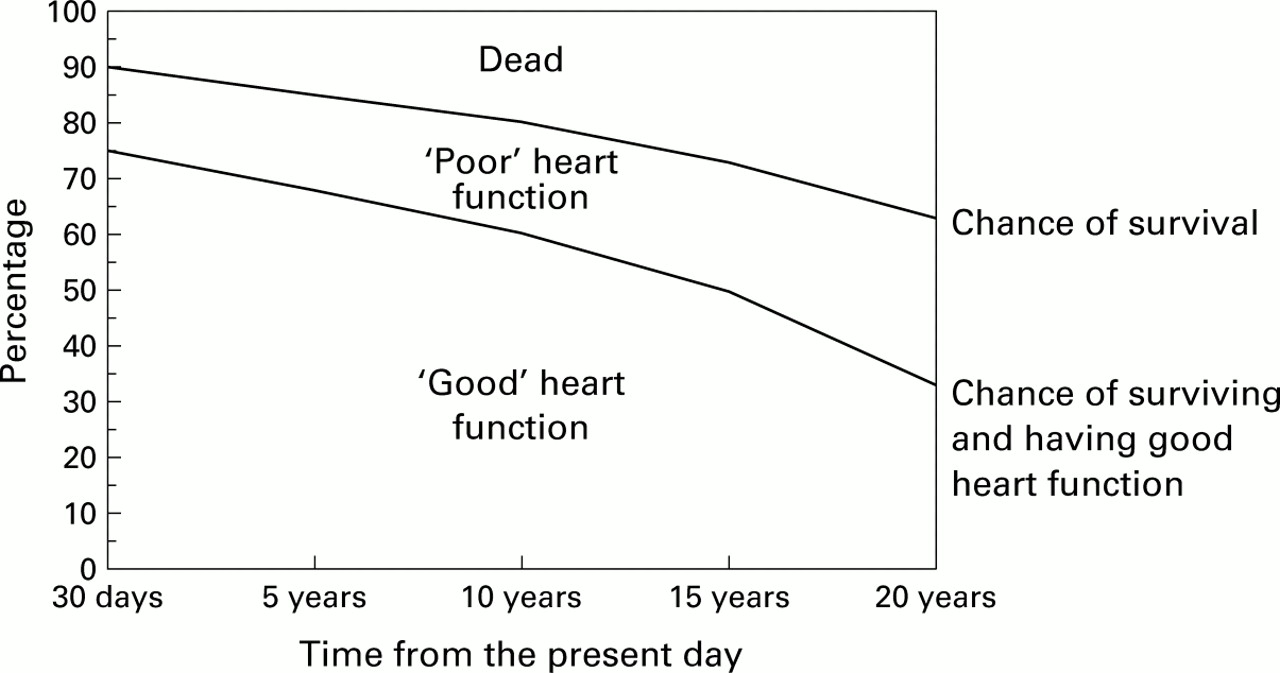
Participants indicated their beliefs about the likely outcomes of each option by completing “subjective multi-state survival graphs” (fig 1). By adding two lines to the grids provided, participants indicated the likelihood of mortality, survival with poor heart function (New York Heart Association (NYHA) functional class I or II), and survival with good heart function (NYHA functional class III or IV) over a 20 year time frame. Participants then rated all four options on a scale from –5 (strongly dislike) to +5 (strongly favour).

{kind=link}
Example of a subjective multi-state survival graph. These were drawn for four patient management options by all participants on the basis of their belief. If the vertical axis is transformed by dividing by 100, the areas correspond to expected years in a given state.
ANALYSIS
Option ratings were recorded to the nearest 0.2 points on the scale. Preference between options was then determined by the difference between ratings, indicating both the direction and magnitude of preference for one option over another. Assigning one stage TCPC as the reference option in all such preference calculations (rating for option minus rating for one stage TCPC), three preference scores were obtained per participant for each patient.
The multi-state survival graphs may be read as subjective estimates of the varying probability over time that each patient is in one of three mutually exclusive and exhaustive states (dead, alive with good heart function, or alive with poor heart function). Outcome probabilities (converting percentages to a scale from 0 to 1) were recorded to the nearest 0.01 at 5 year intervals. Graphs areas were used in preference to point probabilities to record participants' expectations about outcomes, maintaining the continuous nature of the information elicited. The areas of bounded regions on the graph represent the expected number of years in each outcome state. The area under the upper curve represents the expected number of years survival (in this time frame) and, by subtraction, the area above this curve represents the expected number of years that the patient is dead. Similarly, the area under the lower curve represents the expected number of years with good heart function (NYHA I/II) and the area between the upper and lower curves indicates the expected time with poor heart function (NYHA III/IV). The advantage of one option over another with respect to the expected number of years in each state was calculated. One stage TCPC was used as the reference option, resulting in measures indicating both direction and magnitude of advantage concordant with preference measures. For some analyses the time scale was divided into medium term (0–10 years) and long term outcome (10–20 years). This allowed examination of the relative contribution of near future or far future outcomes in explaining option preference. This also permitted consideration of how beliefs about long term outcomes (relative to beliefs about more immediate outcomes) differed with whether doctors encountered GUCH patients. Where incomplete graphs were drawn, data points were not inferred but remained missing data.
Correlation and multiple regression were used to examine which advantage measures (specified by different outcome states and different time frames) were most closely associated with preference measures.
Results
SUBJECTIVE PROBABILITY JUDGEMENTS AND OPTION RATINGS
Option ratings and survival likelihood judgements are summarised in table 1. Patterns of preference for the same patient differed between doctors, as indicated by the range of option rating ranks (1 = most favoured, 4 = least favoured).
Chance of survival and option rating by patient management option and by patient
RELATIONSHIP BETWEEN LIKELIHOOD JUDGEMENTS AND OPTION PREFERENCE
A weak positive correlation (r=0.32, p=0.006) was observed between preference and the difference in expected years survival (over the 20 year time frame). Correlation coefficients (table 2) indicated that preference is more closely associated with survival advantage in the long term than in the medium term (analysis 1). Preference is also more closely associated with differences in the likelihood of survival with good heart function than with survival with poor heart function (analysis 2), or with survival per se. Multiple regression confirmed that the independent contribution of these variables in explaining preference corresponded to this pattern of simple correlations.
Relationship between the subjective probability of outcome states and preference between options
A final multiple regression simultaneously examined the main effects of time and of functional status (analysis 3). Predictor variables were coded to examine the balance between risks (the chance of death) and benefits (the chance of survival with good heart function). Once the advantage with respect to survival with good heart function in the long term is taken into account, differences in the subjective probability of other outcomes are not significantly related to preference.
DIFFERENCES IN JUDGEMENT BY GUCH PRACTICE
Differences in judgement were examined by considering the expected number of years survival and the expected number of years survival with good heart function, with the time frame split at 10 years after surgery. All three surgical options were considered as a single category, providing an appropriate dichotomy for considering how the reporting of surgical outcomes in journal papers may have differential impact on GUCH and non-GUCH practitioners. This also represents a more straightforward approach to considering optimism and pessimism about outcomes than considering each option separately.
Table 3 shows that GUCH practitioners were, in general, more optimistic about outcomes than participants who saw only children. Mean estimates by GUCH practitioners for the expected number of years survival and of years survival with good heart function exceeded those of their colleagues for all combinations of strategy and time frame. Group differences for outcomes without surgery were greater for long term than for medium term outcomes, and group differences for outcomes with surgical intervention were smaller for long term than for medium term outcomes.
Expected outcomes by GUCH status (GUCH practitioner v non-GUCH practitioner) and strategy (no surgery v surgery)
A mixed model ANCOVA was performed on estimated years survival with three factors: GUCH status (GUCH v non-GUCH), strategy (no surgery v surgery), and time frame (medium v long). Booklet (A v B) was entered as a covariate to control for any differences in allocation. There was a significant main effect of GUCH status (F(1,80)=27.9, p<0.001), indicating that GUCH practitioners were more optimistic concerning the likelihood of survival for these patients. There was a statistically significant interaction between GUCH status and strategy (F(1,80)=13.0 , p=0.001). Estimates by GUCH doctors of the likelihood of mortality were more similar for the two strategies, whereas non-GUCH doctors provided higher estimates of the likelihood of survival for surgery than for no surgery. The time × GUCH × strategy interaction approached significance (F(1,80)=3.1, p=0.080). This can be interpreted by considering the likely rate of late attrition, the difference in the likelihood of death between the two time frames. For GUCH doctors the likely rate of late attrition was slightly greater without surgery than with, whereas for non-GUCH doctors the likely rate of late attrition was considerably greater without surgery than with. Exact effect sizes obtained from this analysis should be treated with caution as the variance differs between cells. Some small cell sizes precluded the use of inferential statistics to examine differences in beliefs about the likelihood of good heart function.
Discussion
Doctors varied in their preferred management for the same patient, highlighting the difficulty in identifying the best treatment option where considerable uncertainty exists. Differences in option rating were more closely related to differences in the likelihood of survival with good heart function than to differences in the likelihood of survival per se. These option preferences were also more closely related to the chance of survival in the long term than in the near future. Combining these findings, the likelihood of survival with good heart function in the far future appears to be the most important outcome for determining or justifying option preference. From the perspective of utility theory this implies that, not surprisingly, good heart function represents a more highly valued state of health than poor heart function. More unusually, these results imply that far future life years have greater utility than life years in the immediate future, a finding at odds with many studies of patient preference.13–15 From another theoretical perspective, option preference is consistent with maximising the likelihood of a good outcome in preference to minimising the likelihood of a bad outcome.16
In situations such as the one examined here, where multiple outcome states are possible and the likelihood of these vary over time, the relative value placed on different outcomes will be crucial in determining the preferred option. Health states will differ in value (utility) according to the quality of life they offer (outcome preference) and according to how the near future is valued in relation to the far future (time preference). Ultimately, it is the outcome and time preferences of patients (or, arguably, of parents when they act as proxy decision makers) that should determine choice. Ensuring that patients' preferences are incorporated in the decision process is far from straightforward. In principle a range of strategies can achieve this, though with a decision as complex as the one examined here, there is no easy option. A doctor can attempt to ascertain their patient's outcome and time preferences, and then make a recommendation based on their understanding of the likelihood of different outcomes. At the other end of the spectrum, patients can be informed of the chance of different outcomes and weigh the options accordingly. Shared decision making represents an intermediate approach, amalgamating aspects of both strategies.4
Contrary to some anecdotal reports, GUCH practitioners were more optimistic about outcomes than their colleagues. However, importantly, it was non-GUCH practitioners who were more optimistic concerning outcomes following surgery relative to outcomes if no surgical intervention took place. This difference would be anticipated if the feedback obtained from GUCH practice moderates the optimism expressed in journals concerning outcomes after surgical intervention. This difference was more marked for long term outcomes. Again this could be attributable to differential feedback. All specialists receive feedback for individual patients for immediate and medium term outcomes (via clinic consultations). However, non-GUCH practitioners receive less feedback on individual patients for long term outcomes after surgery, as 10–20 years after an operation it is likely that the monitoring and care of patients has passed to a separate GUCH clinic (in some cases at another centre). Differences in the perceived survival advantage of surgical intervention over non-surgical intervention are greatest where differences in feedback are greatest. Determining which group of practitioners is likely to be more realistic in their long range forecasting is problematic. Certainly, the potential for biased judgement exists regardless of whether published results or personal experience are the primary source of feedback. The selective reporting of results is liable to inflate the proportion of series with (comparatively) better outcomes among those series that are published. Equivalently, there is no guarantee that memory for clinical cases provides an accurate guide to the likelihood of specific outcomes.1718
These findings have important implications for clinical practice. A clear association between belief about likely outcomes and option preference was found. Beliefs about likely outcomes were seen to vary with whether or not doctors see GUCH patients in the course of their clinical or surgical practice. Although causality cannot be definitively established, we might expect that GUCH practitioners would advocate different strategies to their colleagues because they hold different beliefs about the relative efficacy of different options. Moreover, differences in belief about the relative efficacy of options were greatest for longer term outcomes—precisely those outcomes that seem most influential in determining option preference. GUCH patients represent a patient group whose needs and management differ from paediatric congenital heart patients. Where such subspecialties arise, there is always discussion about the benefits of specialisation versus generalisation in practice. This study suggests that systems and practice arising from the resolution of these constraints and debates could have considerable bearing on doctors' preferences for different patient management strategies. In particular, it highlights the importance of having good information about patient outcomes, and ensuring that this is disseminated across all relevant specialties.
The variation in doctors' preferences (reflecting differences in the belief about likely long term outcomes) illustrates the problematic nature of deciding what risk information to provide when the evidence base is limited. Subjective projections about far future outcomes may well be the only option in the absence of hard data on the long term outcomes for recently introduced treatments. Nevertheless, anxiety over using this information as a basis for decision making would be understandable.19
Having decided what information should be provided to inform a patient's consent or decision making, the issue of how to present it must be addressed. Risk information is frequently misinterpreted, forgotten, or, some might argue, simply too complex for people to use effectively.20–23 For situations such as the one examined here, multi-state survival graphs might usefully become part of a varied armoury of aids to patient communication.24 Some evidence suggests that graphical presentation of quantitative information increases the effectiveness of communication.2526 Multi-state survival graphs summarise a lot of information and highlight some aspects that are important for informed consent and decision making. Firstly, they make it explicit that a range of outcomes is possible and could provide a focus for discussing the limitations associated with different states of morbidity. Secondly, these graphs show changes in the probability of outcomes over time, allowing people to consider both immediate and long term risks and benefits of different treatments simultaneously. Thus, the use of multi-state survival graphs in communicating with patients could be explored, examining whether they could be an aid to understanding, memory, and decision making.
This study has sought to examine the clinical impressions that lie behind doctors' treatment recommendations in a situation where there is considerable uncertainty. The results were consistent with doctors placing greater weight on long term than on immediate outcomes, and highlight some of the challenges of involving patients and their families in such decisions.
Acknowledgments
Thanks are due to all those who participated in the study, Dr Kate Bull and Dr Elliot Shinebourne for advice on the design of the study, Dr Ian Sullivan and Dr Philip Rees for assistance with the preparation of patient summaries, Dr Charles Vincent, Dr Nigel Harvey and an anonymous referee for their comments on earlier versions of the paper, and the Medical Research Council for their financial support of this work through a PhD studentship.